Duodenal Switch
The duodenal switch, also known as biliopancreatic diversion with duodenal switch, combines restriction of food intake, by reducing the size of the stomach and reduced absorption of calories through the intestinal wall, called malabsorption. Unlike the gastric bypass however, this is accomplished by a scaled reduction of the size of the stomach and the absorptive capacity of the small bowel. This results in the stomach of the duodenal switch patients to function nearly identical to a normal stomach, but on a smaller scale.
The duodenal switch is performed less frequently than the two major bariatric procedures (gastric bypass, gastric sleeve) however it offers the greatest degree of weight loss potential, combining many of the advantages of gastric bypass while minimizing some of its risks.1
How the DS Works:
In the first part of the procedure, a significant portion of the stomach is cut away along the greater curvature and removed from the abdomen. The remaining, smaller gastric sleeve means that less food can be consumed at any given time. This, in turn, allows the patient to feel fuller sooner. Unlike the gastric bypass, the stomach that is left behind is still functioning as a normal stomach with the pyloric valve in place, where as in the gastric bypass procedure, the pyloric valve is made completely ineffective.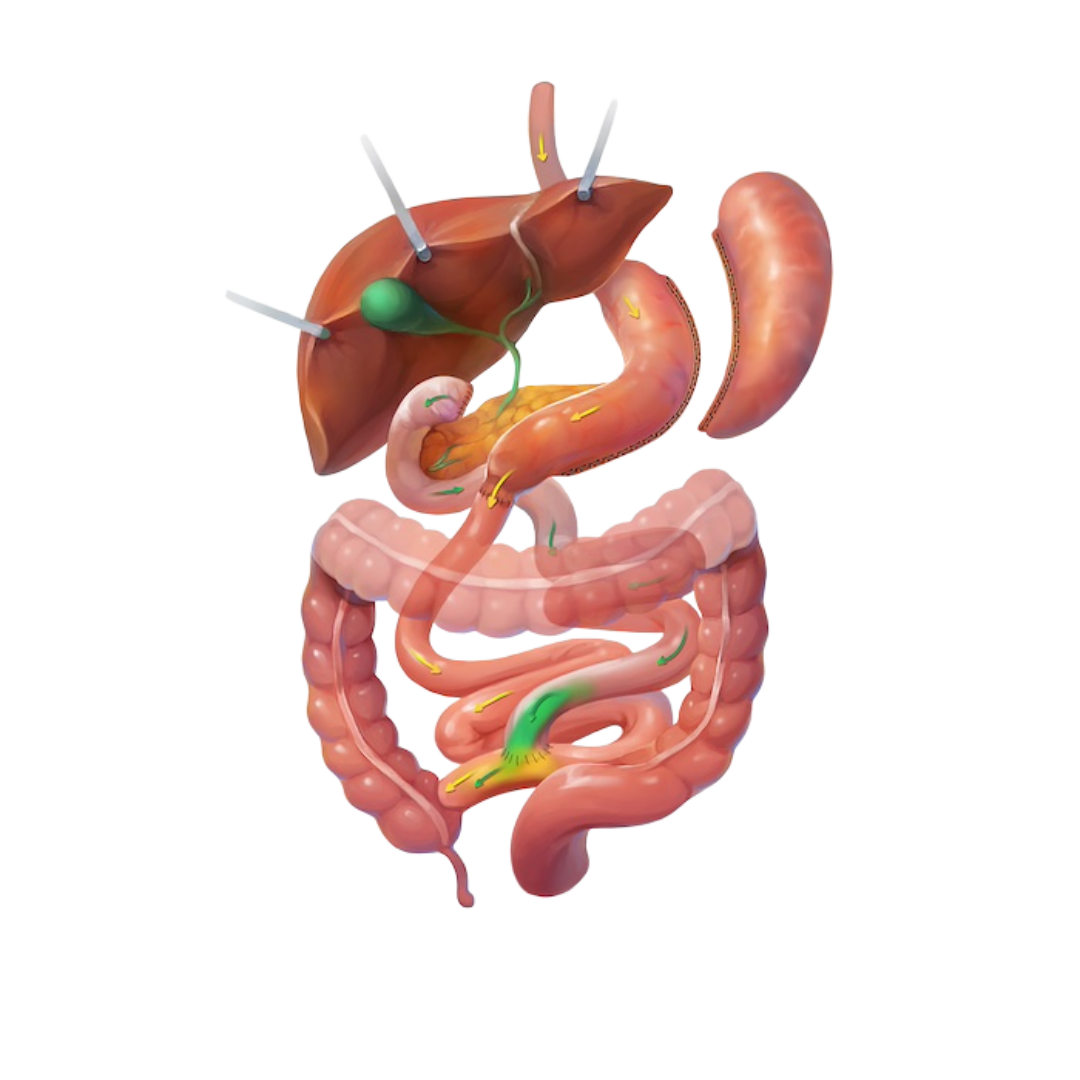
The second part of the surgery, the small intestine is re-routed to create two tubes, one that carries food and the other, bile and pancreatic fluid. Both arrive at a common tube, lower in the digestive tract allowing digestion to continue. The diversion means that there is less surface area for calories to be absorbed into the small intestine walls, reducing the number of calories absorbed. No small bowel is removed during the duodenal switch operation.
The duodenal switch procedure is usually performed in a minimally invasive manner, often leading to a shorter recovery and hospital stay when compared to a traditional open procedure.
Results:
Excess Weight Loss: up to 70%1
Resolution/improvement of type-2 diabetes: up to 98%1
Resolution/improvement of High Cholesterol: up to 99%1
Resolution/improvement of High Blood Pressure: up to 83%1
Resolution/improvement of Sleep Apnea: up to 91%1
Advantages of the Duodenal Switch
As with most commonly performed bariatric surgery procedures, the duodenal switch has many benefits, not the least of which are exceptional excess weight loss results and very good obesity-related disease improvement or resolution rates.1 The duodenal switch was created specifically to offer many of the advantages of gastric bypass, while minimizing many of the risks associated with it. The result is a procedure that, while not as commonly performed as the gastric bypass, offers many similar advantages.
These advantages include:
- Exceptional excess weight loss, often over 70%1
- Exceptional obesity-related disease improvement and resolution1
- No dumping syndrome – common in gastric bypass patients
- Uncommon protein and vitamin deficiencies are managed easily
- The ability to consume regular meals, but in less quantity
- A revisional option for failed Gastric Bypass and adjustable Gastric Banding
Choosing to undergo the duodenal switch, as with any other bariatric procedure, is a very important decision, and it should not be taken lightly. The duodenal switch operation is a major surgery and comes with risks which are partially outlined on our risks of duodenal switch page. To understand these risks fully, you should consult a qualified medical professional.
The advantages of the duodenal switch can be maximized by employing a surgeon who is specialized in this particular procedure and who demonstrates exceptional outcomes. Doing so may allow for greater success over the long-term and, on average, fewer complications.
Patients should attend weight loss surgery information seminars to learn more about the different surgical procedures and make an informed decision about their choice of surgery.
Risks of the Duodenal Switch
As with all other weight loss surgery procedures, the duodenal switch comes with a degree of potential surgical risk. Some of those potential risks and considerations include:
General Surgical Risks
Surgical risk is a possibility with any procedure and may be exacerbated by the patient’s poor health due to obesity. As with any other surgical procedure requiring general anesthesia, uncontrolled high blood pressure, smoking, poorly controlled diabetes and other medical conditions may complicate recovery and increase the risk of complications. Other surgical risk may include: hernias, , bleeding, stroke, heart attack, deep vein thrombosis or blood clots in the legs, pulmonary embolus (blood clots to the lungs) and, though rarely, death.
To learn more about the risks of any surgery please speak to your surgeon. Your surgeon will also be able to explain the possible risks unique to your own medical history and circumstances.
Duodenal Switch Risks and Considerations
- Staple lines created to seal portions of the stomach can leak, requiring emergency surgery.
- Potential injury to the Bilio-pancreatic tree. This is where the duodenum is divided for the “switch” part of the procedure.
- Due to the complexity of the duodenal switch procedure, it should only be performed by experienced surgeons with exceptional outcomes.
- With the exception of the large part of the stomach being removed, the rest of the Duodenal Switch operation is a straightforward surgical procedure to reverse.
- Increased gas or frequent loose bowel movements could be a problem in patients who do not exercise discretion in their diet.
For a more complete overview of the potential risks of the duodenal switch, it is recommended that patients attend one or more of the free weight loss surgery information seminars in their area. Patient knowledge of this potentially life-changing surgery can make the procedure more effective in the long-term.
Speaking to your surgeon and/or primary care physician will offer additional information on suitability of this surgery.
References:
1Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, Schoelles K. Bariatric surgery: a systematic review and meta-analysis, JAMA. 2004 Oct 13;292(14):1724-37
This page was reviewed by
